Offer
Provide additional details about the offer you're running.
FLASHSALE
Time to read 6 min
Fecal calprotectin is one of the very good biomarkers that have drawn much attention for non-invasive gastrointestinal investigation, mainly in terms of its use as a marker for diagnosing and managing IBD.
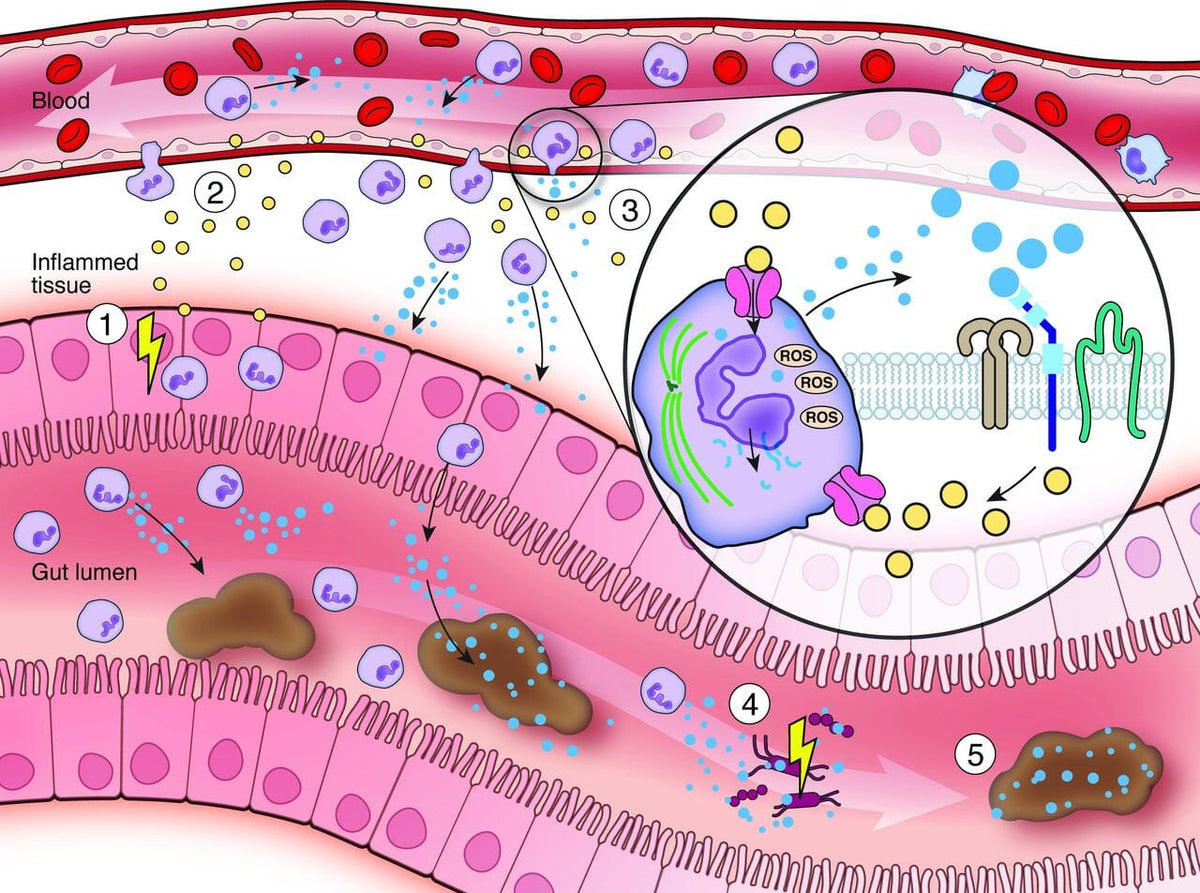
Calprotectin is a protein found within neutrophils, which can be considered a subset of white blood cells.
If the intestines have a condition such as Crohn's disease or ulcerative colitis, white blood cells can penetrate the lining of the intestines and release calprotectin.
This can be measured from a stool sample for its amount in order to diagnose the severity of inflammation of the intestines that separates IBD from other diseases like irritable bowel syndrome (IBS).
Calprotectin is an important biomarker when dealing with inflammation of the intestinal tract, particularly among patients with the condition known as inflammatory bowel disease.
IBD is the umbrella that includes Crohn's and ulcerative colitis, which are chronic conditions causing the inflammation of the gastrointestinal tract.
In both diseases, the inflammation is initiated in the digestive tract but varies in location.
Crohn's disease can affect any part of the gastrointestinal tract from mouth to anus, though it most commonly occurs in the last portion of the small intestine called ileum and the colon.
In contrast, ulcerative colitis involves only the colon and the rectum. In both diseases, inflammation triggers symptoms such as abdominal pain, diarrhea, fatigue, weight loss and malnutrition.
This leads to launching white blood cells by the immune system, which releases more calprotectin in the bowel. High levels of calprotectin are associated with increased inflammation.
Fecal calprotectin is very instrumental in helping clinicians distinguish this disease from other entities characterized by similar symptoms, such as irritable bowel syndrome (IBS).
IBS does not cause visible inflammation in the intestine, whereas a patient with IBD will have obvious mucosal inflammation and thus increased levels of calprotectin in the stool.
Thus, the process of determining the presence of calprotectin in a stool sample is quite useful as an initial test to differentiate IBS from IBD.
The test for fecal calprotectin is non-invasive and rather simple; it can detect intestinal inflammation and monitor the inflammation process.
Essentially, this test is based on a sample of stool containing calprotectin at various concentrations.
Calprotectin is found in white blood cells, which are released when there is an inflammation in the intestines.
Therefore, if calprotectin levels are high, then it means that intestine inflammation is active. This test is of high relevance in the diagnosis and monitoring of inflammatory bowel disease.
The test is useful not only in the diagnosis of IBD but can play a critical role in disease management, thereby tracking calprotectin levels over time to assess disease activity and an appropriate adjustment in the treatment plan.
For example, if the patient's calprotectin levels remain high despite treatment, it may imply that the present therapy is either not effective and adjustment may be necessary.
On the other hand, low levels of calprotectin should be reassuring for both the patient and practitioner and indicate that inflammation is being appropriately managed.
Monitoring may be achieved through assessing the activity of disease by testing levels of calprotectin.
Since IBD is a chronic disease, which during its course tends to evolve through periods of exacerbation and remission, routine follow-up is necessary for effective management of the disease.
Fecal calprotectin is particularly useful in this regard because it directly measures intestinal inflammation.
This is of great importance in assessing treatment efficacy, predicting relapses, and making decisions about further invasive investigations such as colonoscopy.
Additionally, fecal calprotectin may be used not only for monitoring disease activity but also as a predictive tool for relapses in patients with IBD.
Elevated levels often precede the occurrence of apparent clinical signs of a flare-up. In this way, patients having high fecal calprotectin levels are more likely to experience relapse.
The clinical utility of calprotectin includes following patients at risk of relapse so that treatment plans may appropriately be modified before flare-up occurs.
Third, it may help as a decision aid in the escalation and de-escalation of treatment. For example, if a patient's levels are low and steady, then treatment intensity would be reduced.
On the other hand, high sustained calprotectin levels may signify the intensification of treatment to address inflammation and prevent complications.
One of the most challenging distinctions in gastrointestinal disorders' diagnosis is the distinction between irritable bowel syndrome and inflammatory bowel disease.
Both diseases share common symptoms: abdominal pain, diarrhea, and bloating, which makes it pretty difficult to distinguish them based on symptoms only.
In the meanwhile, though, their underlying pathologies are quite different, and this is where fecal calprotectin stands out as a useful diagnostic tool.
In IBD, elevated calprotectin comes from the inflammation present in the bowel, as mentioned above.
By contrast, IBS is not inflammatory in nature. Thus, it is not uncommon for the levels of calprotectin in patients that have IBS to be normal.
The utilization of fecal calprotectin can thus help the clinician determine whether or not a patient's symptoms arise from inflammatory bowel disease or irritable bowel syndrome.
Such a distinction is important because the treatments for IBD are quite different from those for IBS. The drugs used for IBD are anti-inflammatory agents, immune suppressors, or biologic therapies meant to control the inflammation and prevent further complications.
IBS on the other hand is often managed with lifestyle modifications and dietary changes in addition to medications meant to alleviate symptoms rather than treating the inflammation itself. Therefore, accurate identification of the cause of a patient's symptoms would do much in deciding the type of treatment plan chosen.
While this test is very useful in the diagnosis and management of IBD, there are also some limitations.
For instance, increased levels of calprotectin do not particularly indicate IBD; they occur with many conditions that lead to inflammation of the intestine, including infections, colorectal cancer, and NSAIDs use.
So, positive high levels of calprotectin can only indicate the existence of inflammation but cannot be specific to diagnose a patient with IBD.
Moreover, calprotectin levels may differ independently from inflammation. The concentration of this level can be influenced by age, diet, and drugs. It can sometimes also produce false positives and negatives results.
Because of these issues, any result obtained through this test must always be interpreted in the clinical history and symptoms of a patient. No lone measurement of the patient's whole diagnosis is provided by this test.
Despite its weaknesses, fecal calprotectin will likely become an increasingly essential tool for diagnosis and monitoring of gastrointestinal diseases in the future.
Increasing improvement in the accuracy and reliability of the test through advances in technology and research is quite likely to give clinicians additional utility from this test.
Another development that may facilitate easier monitoring of the disease by patients at home is the development of point-of-care fecal calprotectin testing, which can increase testing frequency and lead to earlier detection of flare-ups.
Researchers are further investigating the possibility of using fecal calprotectin with other markers to increase diagnostic precision.
For example, calprotectin alongside markers for gut permeability or microbial dysbiosis might indicate a better reflection of the state of gut health and pathogenesis.
Fecal calprotectin is one of the protein biomarkers used thus far to diagnose and manage inflammatory bowel disease.
The high sensitivity of the test in detecting intestinal inflammation has demonstrated its importance in differentiation from IBS and monitoring or predicting disease activity in IBD.
Although the test is far from being perfect, it is non-invasive; therefore, relatively easy to execute, with respect to value gained from the information related to the health of the gastrointestinal tract.
It is expected that the use of fecal calprotectin will continue to increase with the improvement of the research and development done in the actual technology.
* Medical Disclaimer - The following information is for educational purposes only. No information provided on this website, including text, graphic, and images, are intended as substitutes for professional medical advice. Please consult with your doctor about specific medical advice pertaining to your condition(s).



